The use of ice is currently a rather hot (or should we say cold) debate in the world of sports medicine. Icing has been part of the treatment plan for acute injuries in sport medicine for decades, but the latest research is raising questions over this practice.
The team at ProMOTION spoke to a range of experts to explore the science around the use of ice and the latest research and clinical thinking.
Meet our Panel

What are the current concerns over the use of ice when treating injuries?
Dr Christopher McCarthy:
“Nobody has really considered that there might be a downside to icing people. Well that has been considered here and it’s been shown to be an issue!”
“For most soft tissue injuries, when you look at the size of the actual injury it will be a few millimetres or a centimetre or so, it’s not the whole knee. Everything else I’ve seen, including the good old-fashioned bag of peas over-covers the area; it covers the whole region or a good half of the joint.
Professor James Selfe:
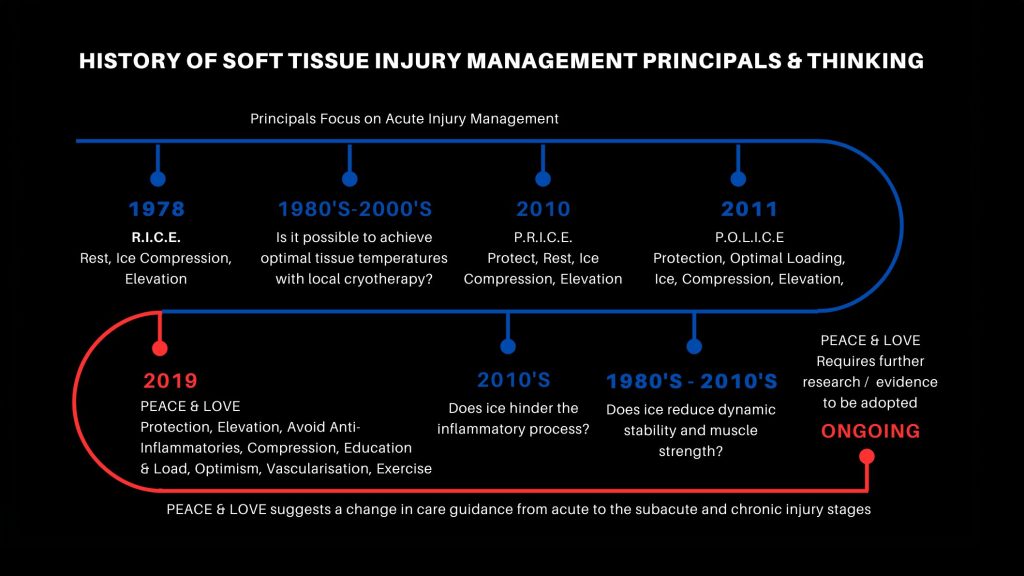
“There are some guidelines which are called the PRICE guidelines, which cover particularly acute injuries. One of the things they talk about is the use of ice, but within the field of cooling there are actually an awful lot of things which are unknown.
“With broad cooling, what happens is you’re getting a shutdown effect of the muscles, so you have less control, less muscle strength. You are actually potentially going to create more problems because you haven’t got the muscle control to then control the joint and the body weight.”
Professor Jim Richards:
“There is a window of treatment that we need. If it is too cold then you’re going to have potential adverse effects, and if it’s not cold enough then you’re not going to have that therapeutic effect. If we look at traditional treatments really, we don’t do that very well.
“When icing using iced water or even gel packs for example, the exact amount of cooling that these are providing is fairly variable.”
How does the ProMOTION EV1 work to counteract these concerns?
Jill Alexander:
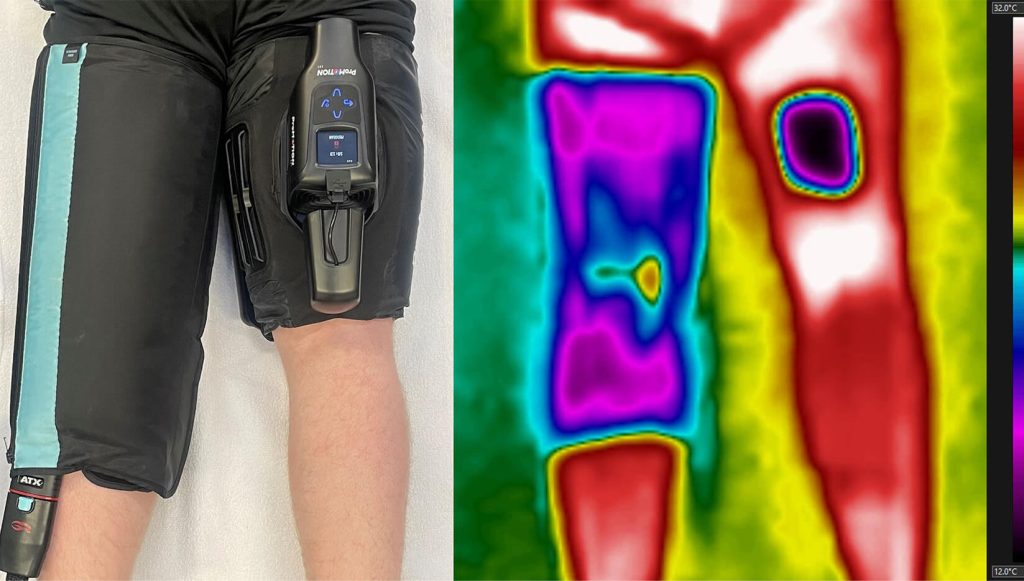
“The targeted effect of this product where we can isolate and cool and area really specific and localised has massive potential for not putting an athlete back on the pitch in a detrimental circumstance.”
Dr Christopher McCarthy, Clinical Fellow, Manchester Metropolitan University
“If you’ve numbed somebody’s knee, their awareness of where the knee is, is a bit less than it was before you put the ice on, so they may be more at risk of having another injury. Whereas if you’ve reduced the pain via a targeted pain relief, then there isn’t that reduction in proprioception (the awareness of where you are in a space) so that’s a real advantage.”
Professor James Selfe:
“If we set the device to 12 degrees, we know we’re going to get 12 degrees and we’ve been able to measure that. And so you’ve created an environment where the healing process can be optimised.”
Professor Jim Richards:
“We can be very targeted in that approach to getting the effects that we want in the area that has been directly affected, but not adversely affect the surrounding areas.”
What does this mean for the practice of using ice in the future?
Professor Jim Richards:
“The particular excitement behind it is the potential to change clinical practice, to offer a new solution. Anything where we can reduce recovery times, improve recovery is absolutely fantastic.”
Where can I learn more?
To find out more about the science behind ProMOTION EV1 and the extensive research that has driven its development click here.